
During the drug development process there are many critical milestones and many more potential pitfalls which could seriously impact the timely progression of a new compound into the next phase. One of the major milestones is the entry into clinical phase 1, where a new compound is administered to healthy subjects for the first time. The greatest challenges arise from the fact that both the synthesis and characterization of the drug substance is still limited and yet clinical material must be produced and released for use in humans. For clinical trials the drug must be converted into a form that has sufficient stability and bioavailability, and at the same time can be provided in an administrable form of different dose strengths. However there are multiple drug characteristics (table 1) which might prevent or at least challenge the provision of clinical materials of an orally administered drug compound for the first in human trials.
Fill in the form to unlock the rest of this content.
During the drug development process there are many critical milestones and many more potential pitfalls which could seriously impact the timely progression of a new compound into the next phase. One of the major milestones is the entry into clinical phase 1, where a new compound is administered to healthy subjects for the first time. The greatest challenges arise from the fact that both the synthesis and characterization of the drug substance is still limited and yet clinical material must be produced and released for use in humans. For clinical trials the drug must be converted into a form that has sufficient stability and bioavailability, and at the same time can be provided in an administrable form of different dose strengths. However there are multiple drug characteristics (table 1) which might prevent or at least challenge the provision of clinical materials of an orally administered drug compound for the first in human trials .
Critical attributes of drug substances
- Poor or pH dependent aqueous solubility
- Poor permeability
- Narrow window of absorption
- High pre-systemic metabolism
- High first pass effect
- Poor crystal formation
- Poor compactability
- Polymorphic changes
- Degradation at gastric pH
- Narrow therapeutic window
List 1: Some of the major drug characteristics which can cause issues in clinical material provision
Consequently the development of a suitable phase 1 clinical formulation and its cGMP manufacturing is a critical milestone and essential for planning and ensuring the first in human clinical trial starts on time. The objective of the phase 1 clinical trials is to establish a pharmacokinetic and safety profile of the drug in healthy volunteers. A dosage form is required that isable to secure sufficient plasma levels and exposure to the systemic circulation as well as to show drug stability during the course of the study.
Development of a phase 1 formulation
Supporting a phase 1 formulation development program should be a balance between different elements such as the performance and quality requirements for a phase 1 formulation, and the necessary pharmaceutical technology approach to achieve this. Ardena uses a rational approach which starts with a thorough review of the available physicochemical characteristics of the drug substance complemented by additional analysis if required. These data support a risk assessment leading to [Figure 1]. In the ideal case the drug compounds can be metered accurately in two-piece hard capsule in the dose strengths required to support the phase 1 clinical trials, however very few drug compounds have suitable characteristics for this and instead require specific formulation development work and drug delivery technologies.
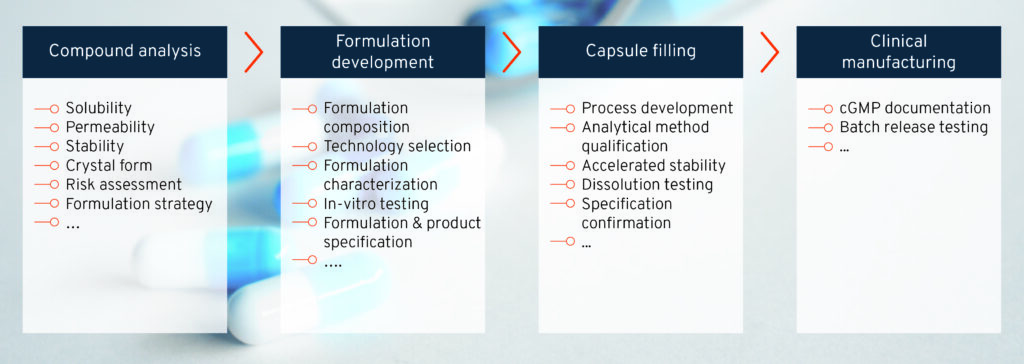
Figure 1: Rational approach for phase 1 clinical drug product development and manufacturing
For the majority of drug substances more extensive formulation development work is required to obtain a clinical product with the desired quality and clinical performance to avoid an inconclusive phase 1 clinical trial or the program having to be put on hold and subsequently repeated with a new, more adequate phase 1 product [1].
Poor aqueous or pH dependent solubility and poor permeability are common properties of new chemical entities [2, 3]. Drug compounds with these characteristics do not achieve sufficient plasma concentrations without the application of solubility enhancing drug delivery technologies. Generally the development of bioenhancing drug delivery formulation and processing is complex and requires resource intensive development programs for the commercial formulation. For clinical phase 1 drug delivery formulations, platform technologies and scientific expertise have evolved enabling drug compounds to reach clinical trials quickly and effectively..
Unfavourable characteristics such as high lipophilicity or high lattice energy can cause molecules to have poor aqueous solubility For drug compounds with high lipophilicity determined by logP, clogP or logD7.4 lipid-based formulation can be considered. Such formulations need to be developed on scientific grounds and should employ a rational selection of a lipophilic phase with or without surfactants or cosolvents such as polyethylene glycol. In such systems the drug compound is dissolved or dispersed, enhancing the bioavailability for example through the formation of supersaturation during lipid dispersion or digestion [4].
For drug compounds with poor aqueous solubility, for example due to a high lattice energy or molecular weight beyond 500 Da, the bioavailability can be influenced by increasing the rate of dissolution which is dependent on the surface area and the physical form of the drug.
A substantial increase of the drug surface area exposed to the aqueous phase and the dissolution rate can be achieved by reducing the particle size e.g., by micronization or nanotization. Since particle size reduction is accompanied by particle charging and agglomeration, the milling process must be carefully selected and the micronized or nanosized drug generally requires the support of formulation with functional excipients like wetting agents, disintegrants and glidants [5].
By changing the physical state from crystalline to amorphous, the drug is transferred into a thermodynamic state where the intra-molecular forces in its crystalline state are reduced and inter molecular hydrogen bonds with water increase. When stabilized into their amorphous states, drug compounds show an increase in kinetic solubility and can form metastable supersaturated solutions which translates into an increased in-vivo rate of absorption [6]. To convert a crystalline compound into its amorphous form two major pharmaceutical technologies able to generate a solid dispersion are used: spray drying and hot melt extrusion.
In the spray drying process the compound is dissolved together with polymers in solvent and then atomized by spraying into small droplets, which dry instantaneously to form distinct solid microparticles of the amorphous drug stabilized by the polymer [8].
In a hot melt extrusion process (HME), the compound is mixed with polymeric excipients and heated above the glass transition temperature until molecular mixing is achieved where the compound is embedded in the polymer matrix in its amorphous form and solidifies by cooling [7].
Over the past decades we have gained a good understanding of the mechanisms of HME and spray drying process technology along with several successful product launches using each. Spray drying provides some advantages over HME including better particle size reduction, higher porosity and better wettability, which are favorable from the early development and phase 1 clinical supply perspective [9].
Development of a phase 1 dosage form
To orally administer the drug and its formulation in the phase 1 clinical program, different dose strengths in a single dosage form unit are required. Additional excipients (e.g., binders, diluents, disintegrants, wetting agents, glidants) and processing steps (e.g., wet/dry granulation, compression, coating) are often required for oral dosage forms which can add unnecessary complexity and potential risks for stability or performance issues to the phase 1 manufacturing and supply [10]. While tablets are the most common oral dosage form with established manufacturing processes, there are some important factors that are not favorable for the tablet dosage form in the early clinical trials. Tablet manufacturing requires a drug powder blend with excellent flow properties on the machines to achieve content uniformity for which in most cases an additional granulation process (e.g., dry or wet granulation) is needed. Drug compounds generally have an unpalatable flavour, requiring a taste masking coat on the tablet. The disintegration and dissolution of the tablet are driven by its porosity which is dependent on the powder properties, the compression forces and profile applied, and the coating. To keep the phase 1 formulation as simple as possible, two-piece capsule technology has emerged as the dosage form of choice due to their ability to dose drug compounds or microparticles with poor flow properties, their provision of effective taste masking and retention of the dissolution characteristics of drug compound formulation in the absence of a strong powder compression step [11, 12]. In addition the application of capsule technology for complex compounds and delivery forms has been greatly expanded by the introduction of new capsule polymers (e.g. HPMC) and filling technologies.
Analytical characterization and in vitro-dissolution
Analytical characterization is an essential part of clinical product development and manufacturing as this builds the basis of the product release specification which is mandatory for the IND or IMPD filing. Accurate analytical methods for drug compound stability, impurities, content uniformity, drug dissolution and other quality criteria are needed to fulfill these regulatory requirements. From a phase 1 product development perspective in-vitro dissolution tools play a particularly important role in the formulation and dosage form selection process. The in-vitro tools may also include predictive methods with biorelevant or discriminatory dissolution media or different dissolution apparatus in order to confirm the assumptions made during the drug compound assessment and definition of the most suitable clinical product development approach [13].
Beyond oral small molecules
The emerging clinical investigations of life biotherapeutics create distinct challenges for entry into phase 1 clinical trials. For example, probiotics are live microorganisms which are very sensitive to water activity, heat and oxygen and need to be stabilized for pharmaceutical applications. Two major techniques are being used: micro-encapsulation into polymeric systems and controlled removal of water. Micro-encapsulation of a probiotic requires intense investigations into suitable techniques, biopolymers and micro-encapsulation processes, which is similar to freeze drying or lyophilization technologies operating at freezing temperature and low pressure (vacuum). In contrast to these techniques, spray drying has emerged as the technology of choice due to the low energy consumption, lower operational costs, high yield, industrial feasibility, and continuous manufacturing. Experienced scientists can easily adjust the spray drying process using temperature, feed rate, drying time and drying medium to obtain the desired probiotic stability [14]. While tableting of probiotics has become a feasible option, the selection of the necessary excipients is of utmost importance for the compression of probiotics into tablets. The excipients need to be screened for each strain of probiotics regarding their suitability and stabilizing effects as no predictions can be made [14]. While this might be justifiable for the phase 3 and commercial formulation, encapsulation of the conditioned probiotics or spray dried probiotics in moisture reduced HPMC capsule avoids the intensive development and formulation work for the phase 1 clinical trials.
Pulmonary drug delivery is gaining increasing importance for local and systemic application of small molecules and biotherapeutics. They present another challenge for phase 1 clinical trials due to the need for a performance critical device component. Particles for pulmonary delivery must have a particle size < 5µm and need to be metered at very low doses into administration dose units. Such formulations typically consist of micronized drug attached to carriers (e.g., lactose) or engineered particles derived from spray drying technologies. Capsule-based inhalation devices are considered to be the technology of choice for phase 1 and beyond due to the existing expertise in inhalation powder development and processing, and availability of encapsulation equipment able to handle even cohesive powders. [15].
There is growing evidence for the benefit of fixed dose combination products, combining 2 or more different drugs or release profiles into a single unit. Clinical studies for combination products are more complex as they need to identify the contributions of each drug to the overall clinical benefit of the combination [16]. The individual drugs used are established, therefore the program will start with phase 2 trials to provide the clinical proof of concept (cPoC). The challenge for clinical manufacturing is the need for a variety of different combinations and dose strengths to be prepared and blinded. To avoid unnecessary formulation and product development work for this initial trial, distinct product units (e.g., powder mixtures, tablets, etc) are filled into a single capsule to support the variety of fixed dose combinations required for the cPoC [17].
Conclusion
Understanding the various constraints of the early development phases, in particular the “first in human” study, the formulation, dosage form and analytical method development, Ardena consistently employs its “phase-appropriate” approach to efficiently provide the necessary evidence and confidence at each decision point. This applies to drug compounds beyond small molecules such as biotherapeutics and to dosage forms beyond oral delivery such as pulmonary drug delivery as well as complex drug products such as fixed dose combinations or drug compounds with special handling requirements (e.g., OEB 3 & 4 compounds, microdosing). Supported by the required documentation, the clinical batch is manufactured and supplied ahead of the start of the phase 1 trials.
References
- Boyd, B.J. et al (2019) Successful oral delivery of poorly water-soluble drugs both depends on the intraluminal behavior of drugs and of appropriate advanced drug delivery systems. Eur J Pharm Sci 137:104967
- Shulz, M.D. (2019) Two Decades under the Influence of the Rule of Five and the Changing Properties of Approved Oral Drugs. J Med Chem 62:1701-1714
- Brown, D.G. & Wobst, H.J. (2021) A Decade of FDA-Approved Drugs (2010-2019): Trends and Future Directions. J Med Chem 64:2312-2338
- Ditzinger, J. et al (2019) Lipophilicity and hydrophobicity considerations in bio-enabling oral formulations approaches – a PEARRL review. J Pharm Pharmacol 71:464–482
- Wu, D. & Sarsfield, B.A. (2018) Particle Size Reduction: From Microsizing to Nanosizing. In: Early Drug Development: Bringing a Preclinical Candidate to the Clinic, Volume 1, Ed: Giordanetto, F. Wiley‐VCH Verlag GmbH & Co. KGaA
- Iyer, R., et al (2021) Amorphous Solid Dispersions (ASDs): The Influence of Material Properties, Manufacturing Processes and Analytical Technologies in Drug Product Development. Pharmaceutics 13:1682
- Simões, M.F., et al (2021) Hot-Melt Extrusion: a Roadmap for Product Development. AAPS PharmSciTech 22:184
- Davis, M. & Walker, G. (2018) Recent strategies in spray drying for the enhanced bioavailability of poorly water-soluble drugs. J Contr Rel 269:110-127
- Vasconcelos, T., et al (2016) Amorphous solid dispersions: Rational selection of a manufacturing process. Adv Drug Del Rev 100:85-101
- Markl, D. & Zeitler, J.A. (2017) A Review of Disintegration Mechanisms and Measurement Techniques. Pharm Res 34(5): 890–917
- Esseku, F. et al. (2010) The Effect of Overencapsulation on Disintegration and Dissolution. Pharm Technol 4:104-111
- Wilding, I.R. et al (2005) In vivo disintegration profiles of encapsulated and non-encapsulated sumatriptan: gamma scintigraphy in healthy volunteers. J. Clin. Pharmacol. 45(1):101-105
- Mann, J. et al. (2017) Validation of Dissolution Testing with Biorelevant Media: An OrBiTo Study. Mol Pharmaceutics 14:4192-4201
- Gurram, S., et al. (2021) Insights on the Critical Parameters Affecting the Probiotic Viability During Stabilization Process and Formulation Development. AAPS PharmSciTech 22:156
- Stegemann, S. et al. (2022) Focusing on powder processing in dry powder inhalation product development, manufacturing and performance. Int J Pharm 614:121445
- EMA (2017) Guideline on clinical development of fixed combination medicinal products. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-fixed-combination-medicinal-products-revision-2_en.pdf
- g., https://www.mg2.it/processing/capsule-fillers/
