Case study: Building discriminatory power into dissolution testing in late development – a key milestone for the fast product approval
Dissolution testing was introduced into pharmaceutical practice after the occurrence of serious side effects of phenytoin after calcium sulfate was replaced by lactose. As a result, the FDA introduced the USP Dissolution type 1 (Basket method) test as a QC test in 1971 followed by USP Dissolution type 2 (Paddle method) test in 1978. Over the years, FDA developed further guidance to advance in-vitro dissolution testing into an important tool for development, quality control and drug approval. Statistical methods were implemented to compare the similarity or dissimilarity between two dissolution profiles, bio-relevant media were requested for predicting IVIVC and more specific guidelines were release for immediate and modified release products as well as the solubility and permeability characteristics of the drugs according to the BCS drug classification. With the growing knowledge on biopharmaceutics and predictive in-silico tools, dissolution testing has evolved into a key element for drug development and regulatory assessments. This includes that the dissolution test method has to include clinically relevant dissolution specification and must have proven discriminating power between variations outside the acceptance criteria.
Building discriminatory power into dissolution testing in late development – a key milestone for the fast product approval
Dissolution testing was introduced into pharmaceutical practice after the occurrence of serious side effects of phenytoin after calcium sulfate was replaced by lactose [1]. As a result, the FDA introduced the USP Dissolution type 1 (Basket method) test as a QC test in 1971 followed by USP Dissolution type 2 (Paddle method) test in 1978. Over the years, FDA developed further guidance to advance in-vitro dissolution testing into an important tool for development, quality control and drug approval. Statistical methods were implemented to compare the similarity or dissimilarity between two dissolution profiles, bio-relevant media were requested for predicting IVIVC and more specific guidelines were release for immediate and modified release products as well as the solubility and permeability characteristics of the drugs according to the BCS drug classification [2]. With the growing knowledge on biopharmaceutics and predictive in-silico tools, dissolution testing has evolved into a key element for drug development and regulatory assessments [3, 4]. This includes that the dissolution test method has to include clinically relevant dissolution specification [5] and must have proven discriminating power between variations outside the acceptance criteria [6].
Under increasing time pressure in the early development (e.g. phase 1) of new drugs, enhanced therapeutics (e.g. 505(b)(2)) or generics, the development of appropriate dissolution test methods is often limited to determine an adequate dissolution media, which provides sink conditions across the entire dose range of the product. Developing a predictive and discriminatory dissolution test method following the first in human trials has to be considered essential for rapid development of the pivotal clinical trial samples, commercial formulation, the regulatory filing and efficient commercial manufacturing. The earlier this important milestone is achieved in the development phase, the faster and more reliably approval and commercialization will occur [7].
Case study
A known small molecule with a water solubility > 1 mg/ml showed promising results to slow down the progression of multiple sclerosis at a dose of 100 mg tid. The product was formulated as an immediate release capsule. For the phase 1 clinical trial the standard USP type 2 (paddle) dissolution test method with a pH adjusted buffer was used to prove consistent dissolution between the development and the clinical batch. During pre-NDA discussions, the FDA challenged the existing dissolution test and requested evidence that the dissolution method chosen had sufficient discriminating power to assure that the product specification and hence critical clinical performance criteria are met.
Based on Ardena’s expertise a pragmatic, yet rational and systematic scientific approach was defined to develop the discriminatory dissolution method in due time. An assessment on the critical material attributes and critical process parameter of the product led to the manufacturing of 9 aberrant small batches serving for comparison to the clinical phase 1 batch as a reference. The available data from the existing dissolution method were analyzed to select potential dissolution media for the dissolution screen of the 10 different samples. The similarity factor (ƒ2) test was applied to the dissolution profiles of the batches to the reference batch at each time interval. The results demonstrated high sensitivity for one dissolution media discriminating between batches. . In a final design of experiments, the dissolution method was further fine-tuned by modifying the dissolution test procedural parameter (e.g. paddle speed) for the most discriminating power using again the similarity factor (ƒ2) test according to the FDA guidelines [7]. With the newly developed discriminating dissolution test method, 3 of the aberrant batches were found outside the similarity specification providing important understanding on the product and process parameter required to consistently meet the quality criteria of the product.
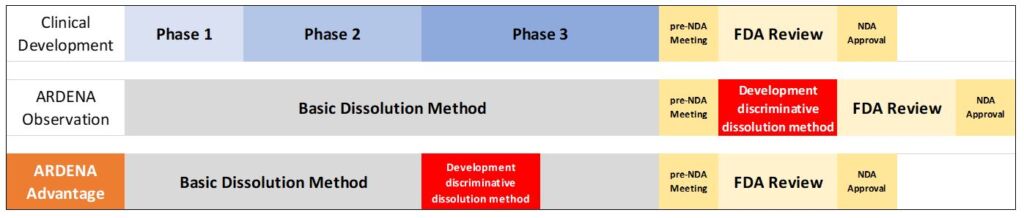
Development of discriminative dissolution method during phase 3 results in 3-6 months time win
While the project passed all IND phases successfully without any further delay, the discriminatory dissolution test revealed important formulation factors like composition, excipients grades and processing affecting the dissolution of the active. This confirms that a discriminating dissolution method available in late phase 2 or early phase 3 of the project, can accelerate the NDA process by 3 to 6 months . Partnering with Ardena’s expertise and scientific resources covering the entire development cycle into the clinics and beyond can mitigate the risk to reach the clinical proof of concept and regulatory approval on schedule.
References
- Tyrer et al (1970) Outbreak of anticonvulsant intoxication in an Australian city. Med. J. 4 (5730), 271–273
- Amidon et al (2006) A Theoretical Basis for a Biopharmaceutic Drug Classification: The Correlation in Vitro Drug Product Dissolution and in Vivo Pharm Res, 12 (3), 413–420
- EMA (2012) Guideline on quality of oral modified release products EMA/492713/2012
- FDA (2017) Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System. Guidance for Industry
- Heimbach et al (2019) Dissolution and Translational Modeling Strategies Toward Establishing an In Vitro-In Vivo Link—a Workshop Summary Report. AAPS J 21:29
- Gray (2018) Power of the Dissolution Test in Distinguishing a Change in Dosage Form Critical Quality Attributes. AAPS PharmSciTech 19(8): 3328.3332
- McAllister et al (2020) Developing Clinically Relevant Dissolution Specifications for Oral Drug Products—Industrial and Regulatory Perspectives. Pharmaceutics 12: 19 (2020)].
- FDA (1997) Dissolution Testing of Immediate Release Solid Oral Dosage Forms; Guidance for Industry
